A Collaborative Digital Space for Global Prosthetics Research and Innovation
Project Summary
Client
Nia Technologies is a Canadian not-for-profit enterprise focussed on designing and developing innovative technologies to improve lives across the globe.
Core Design Team
- Shannah Segal Design Director
- Adie Margineanu UX Designer and Researcher
- Melissa Banyard Visual Designer
Core Client Team
- Jerry Evans President and CEO
- Matt Ratto Chief Science Officer
- Kathleen Gotts Senior Communications Manager
- Danielle Klein UX Intern
- David Singh Product Support Specialist
Activities
- Requirements Gathering
- Stakeholder Interviews
- User Interviews
- Usability Testing
- Workshops & Co-Creation
- User Flows
- Journey Mapping
- Wireframing
- Prototyping
- Visual Design
01
Project-Specific Goals
3D PrintAbility is a digital toolchain designed by Nia to speed up and improve the experience of children requiring prosthetics in low-income countries. It allows prosthetic technicians to quickly create digital molds and print 3D models of the prosthetic socket from limb scans rather than labouring over plaster casts and molds. The results include reduced production time, better access to mobility devices for people with disabilities, and better fitting devices.
With the introduction of the 3D PrintAbility toolchain in pilot studies in Uganda and Cambodia, Nia understands the importance of visibility and collaboration in prosthetic practice and innovation. Specifically, Nia aims to provide digital access to established and innovative prosthetic solutions for practitioners, funding agencies, and rehabilitation centers worldwide. The Usability Matters team was enlisted to provide product vision, strategy, and design for this digital space.
02
Understanding the Problem Space and Generative Research
In order to inform a strategy and vision for this brand new platform, we conducted:
- ARequirements gathering workshops with our client, including stakeholder matrix and content requirements.
- B Remote and in-person stakeholder interviews with prosthetist/orthotist researchers, hospital administrators, funding organization representatives, and clinicians at the point of care in Uganda.
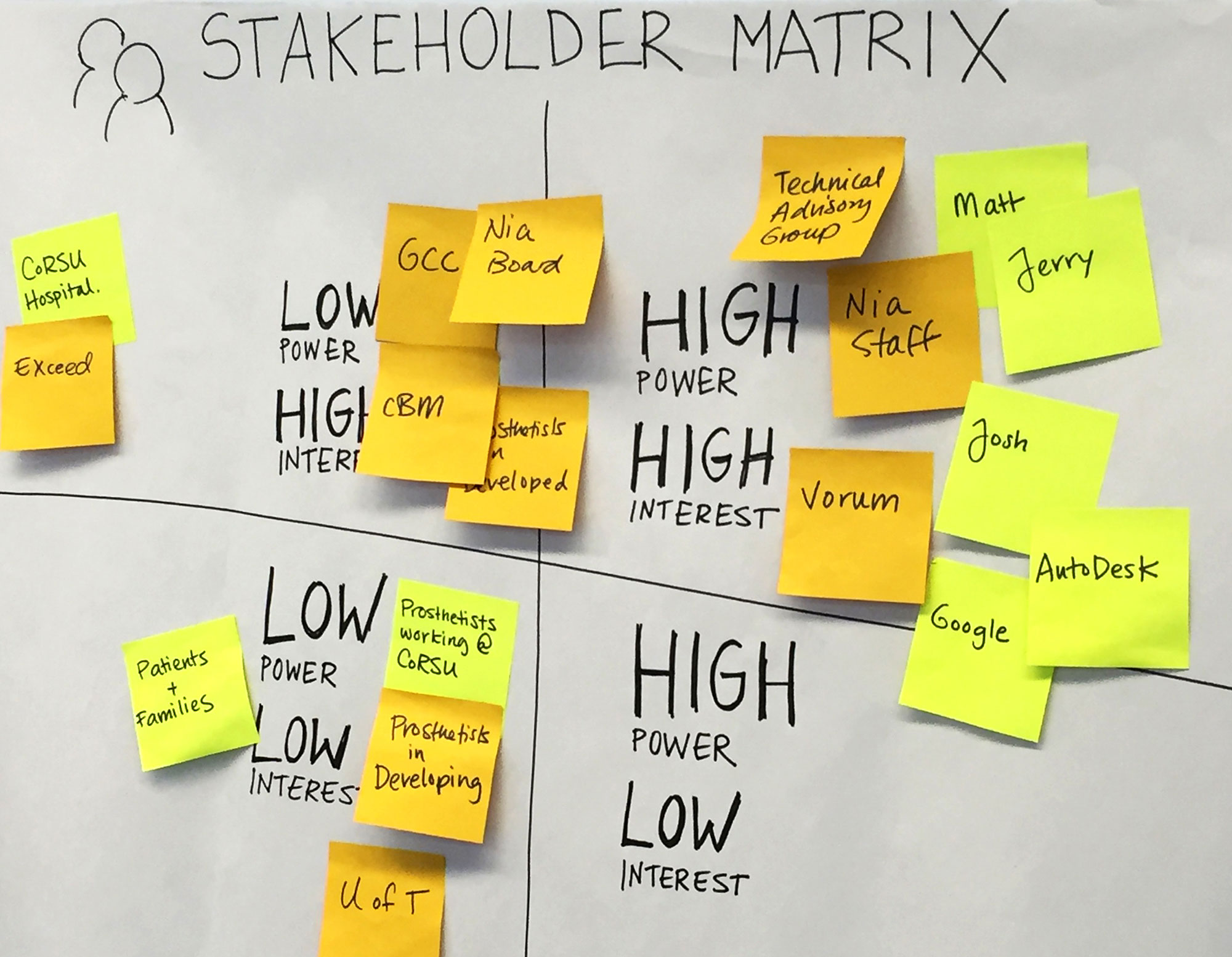
Figure 2.1
A stakeholder matrix helps identify who should be consulted and when during an engagement with diverse and siloed stakeholders and potentially conflicting priorities/needs.
Understanding who has a lot of influence and their interest levels in the project can help us strategize how we communicate and build rapport with them.
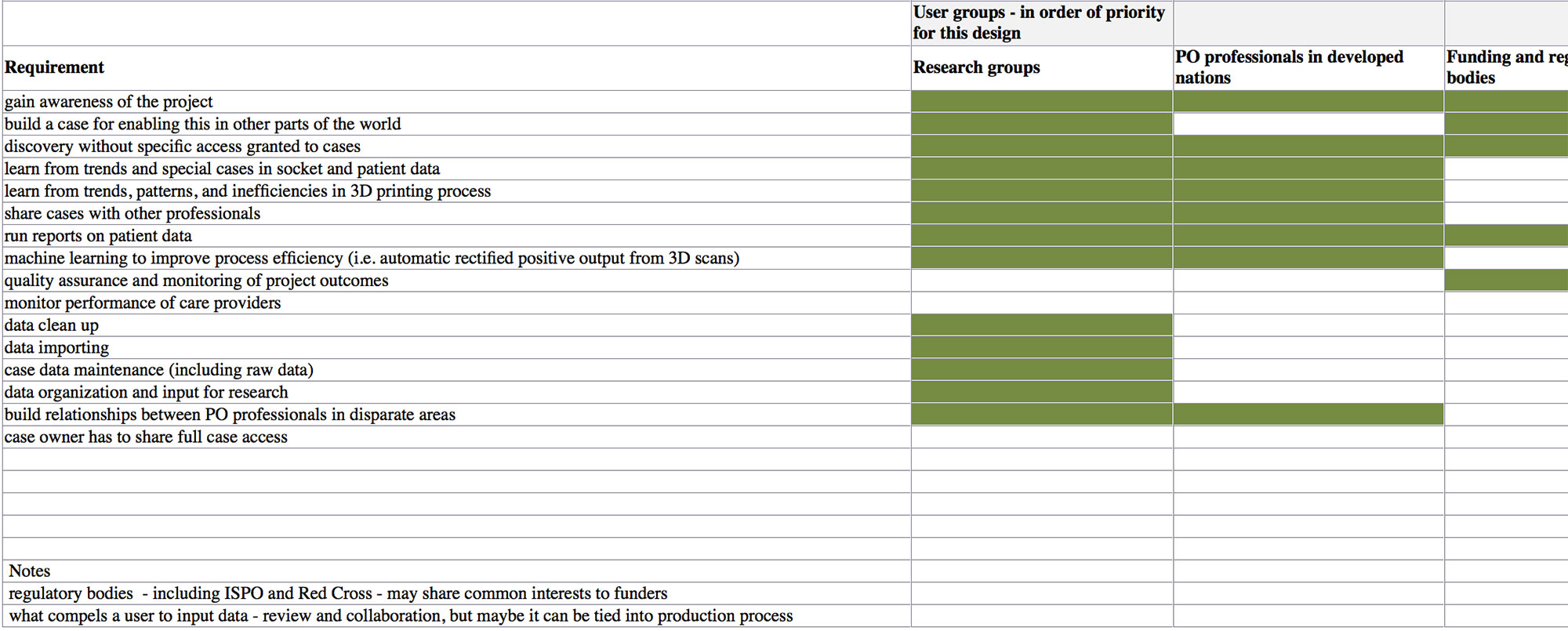
Figure 2.2
Our design would need to address the needs of at least 4 diverse user groups, prioritized based on their power/influence over the project.
To make sure we kept their needs top of mind, we mapped out which project requirement was relevant to each user group (in green).
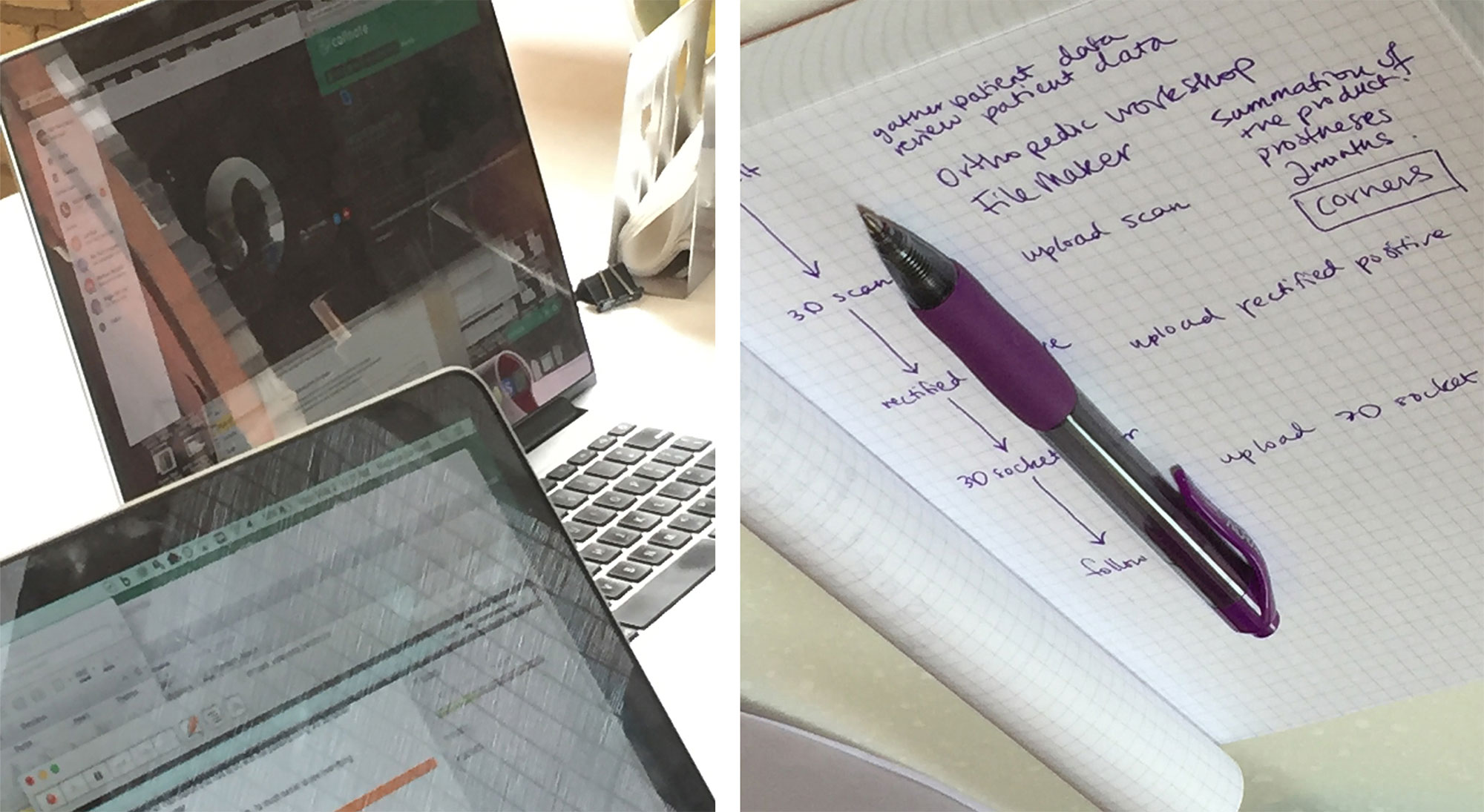
Figure 2.3
Notes and interview photographs from our remote interview with Moses, a prosthetic technologist at CoRSU in Uganda.
He said that the new digital process - while faster - has a lot of "corners" that he needs regular support and expertise from the Nia Team to address.
Generative Research Insights
This truly would be the first collaborative digital platform in the prosthetist/orthotist research space. Most practitioners and researchers indicated that they are used to leveraging their large network of colleagues as the main source of knowledge and continued learning.
The data researchers are looking for is far more robust and requires more meticulous documentation than we anticipated and it is at odds with the data that clinicians at the point of care in Uganda have the time or motivation to input. Researchers and funders are looking for detailed intervention outcomes including videos, images, anatomical measurements, and analysis of walking gait to assess intervention success remotely. Clinicians at the point of care want a patient records management system to easily find patient files, patient treatment history, and be able to input minimal data quickly, easily, and with helpful prompts.
Highlight
The driving force for this platform is data entry at the point of care, so serving the needs of the prosthetic technologists at the point of care is crucial in order for researchers and funding bodies to derive meaningful insights from it.
With this design paradox established, we presented to the larger stakeholder team, finalized a feature set, and created a practitioner at point of care journey map to identify current pain points and potential opportunities the tool could address to incentivise data entry.
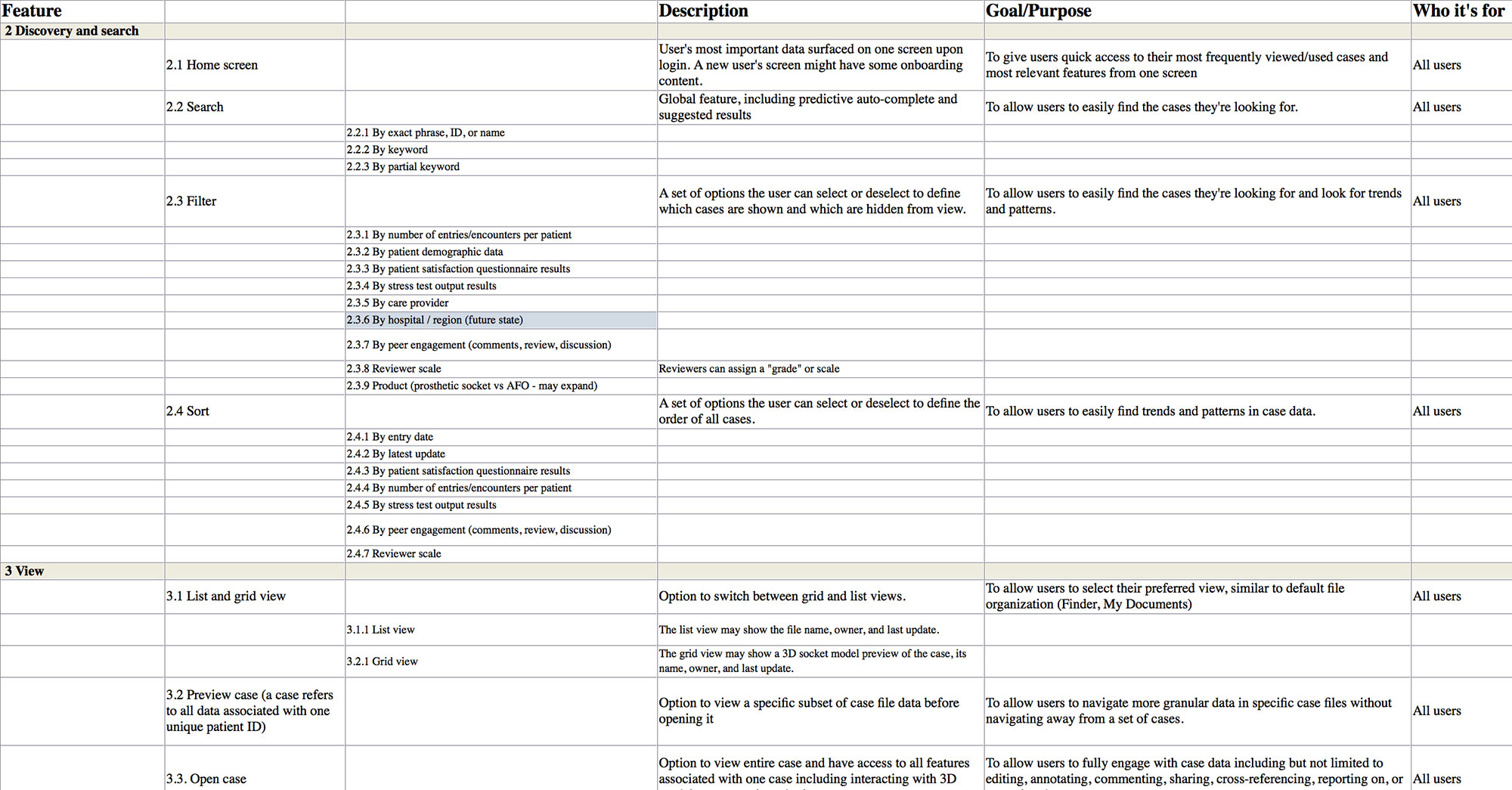
Figure 2.4
Comprehensive feature set of all features to be designed and incorporated into the prosthetics data platform. In order to make this a minimum viable product and focus on the highest value features, we provided a goal/purpose statement for all features or groups of features.
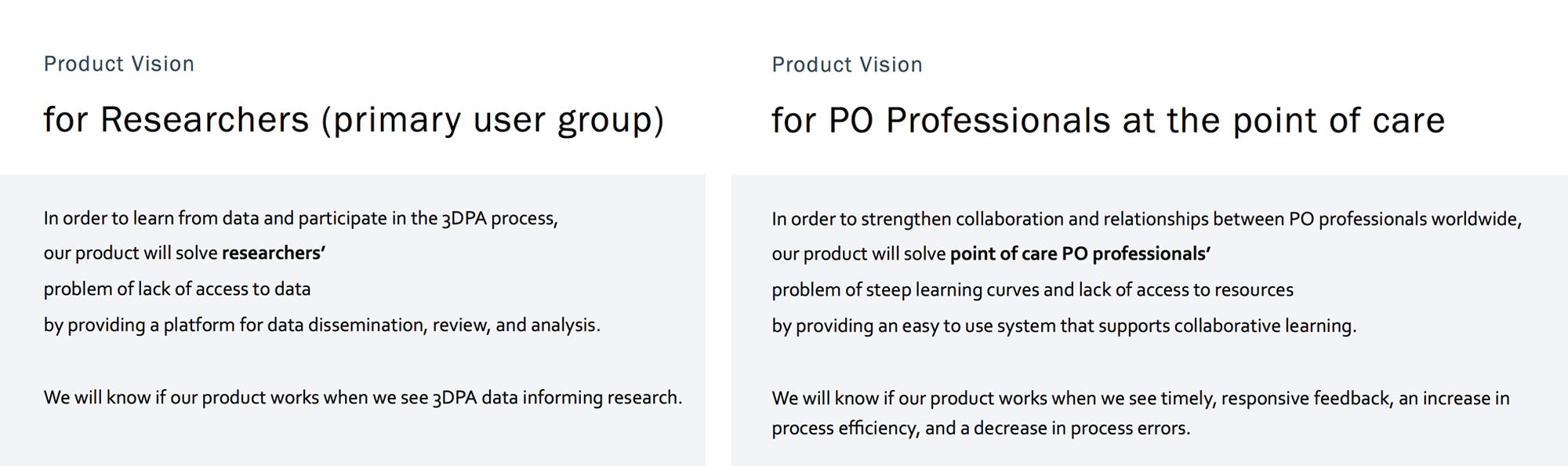
Figure 2.5
Product design visioning exercise that clarifies the problem and needs our product will address for our specific user groups.
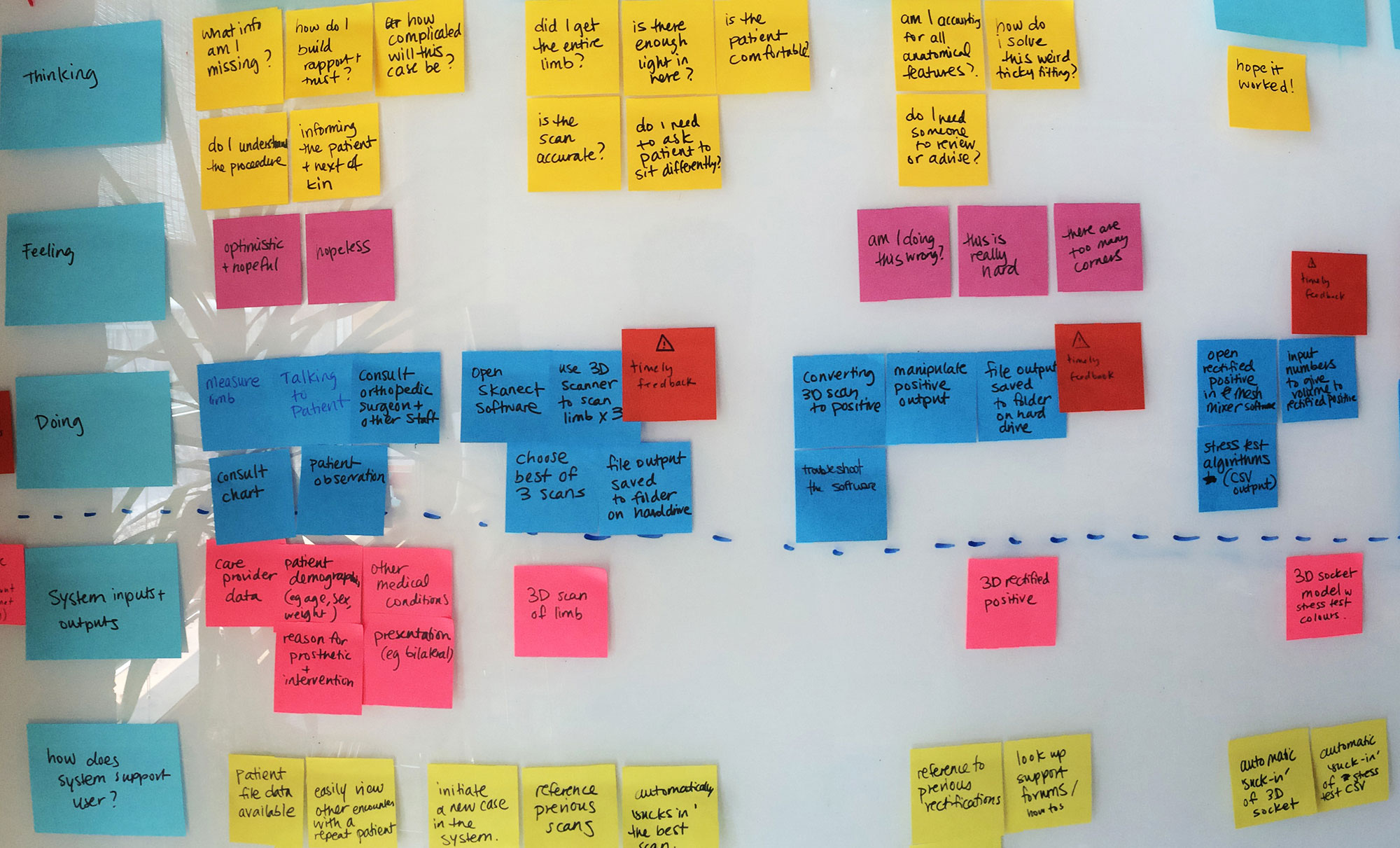
Figure 2.6
Data entry at the point of care is crucial for the usefulness of the prosthetics platform.
We went through the process that the prosthetic technologist goes through during patient consultation, prosthetic socket production/fitting, and after-care/follow up to identify how our design could support their process and incentivise data entry.
Incentives include giving a care provider insight into their own as well as peers’ interventions, an easy way to find patient information, and instant access to other system users for support.
Essential data entry features include streamlining forms as much as possible with minimal open fields and ensuring an instance of the platform works without internet connection loading data asynchronously as internet connection becomes available.
03
The Design Process
The core working team held weekly collaborative sketching sessions in the beginning of the design phase to synthesize the results of the generative research and map out user flows as well as individual screens.
These sketches were developed into a low fidelity interactive Axure prototype in order to test locally and on-site in Uganda with real users.
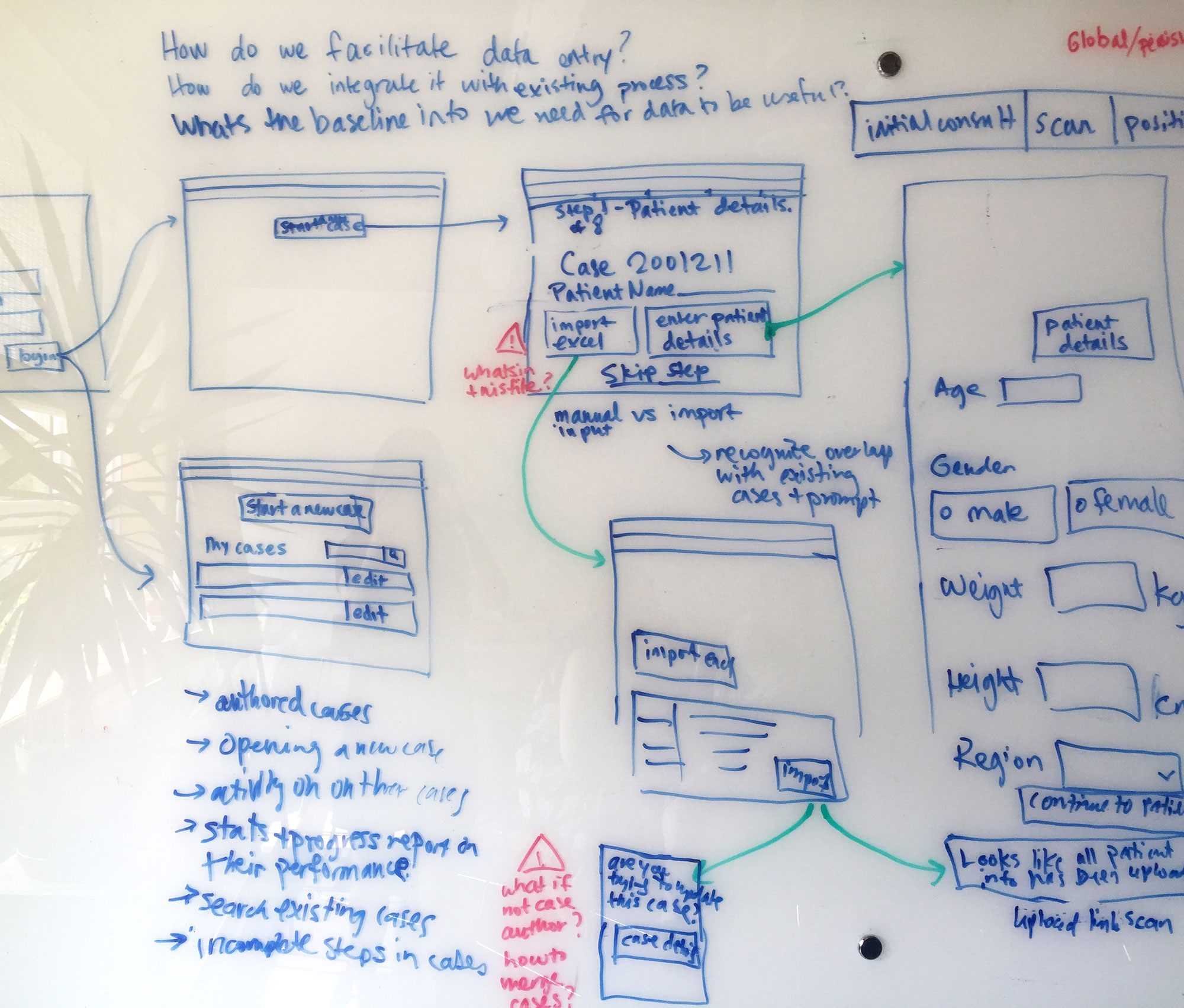
Figure 3.1
Collaborative sketching session of the data entry at the point of care user flow.
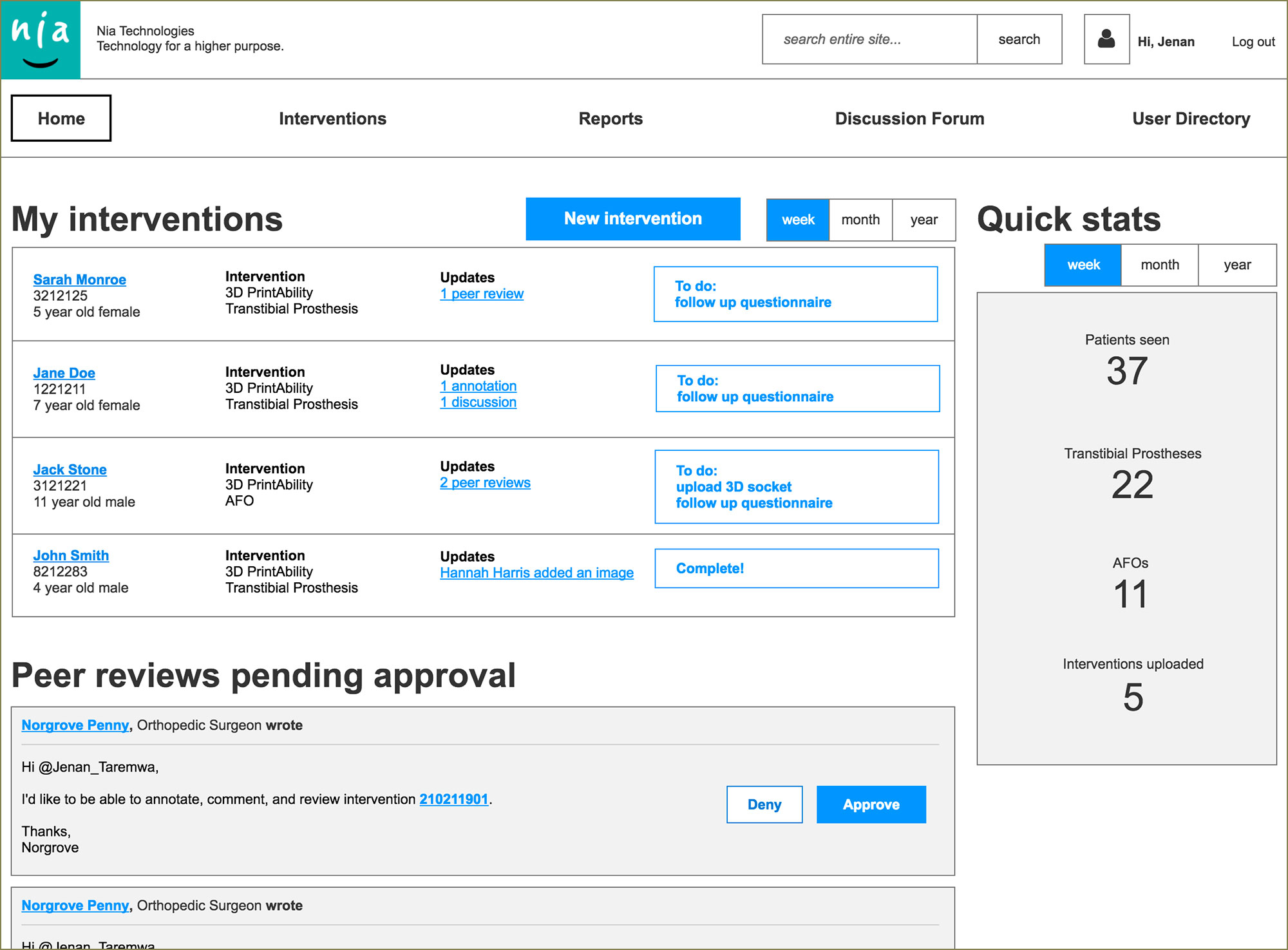
Figure 3.2
A practitioner at the point of care’s home screen as prototyped in the low fidelity Axure prototype.
A researcher’s or a funding organization’s home screen would have variations on the modules and functionality shown here.
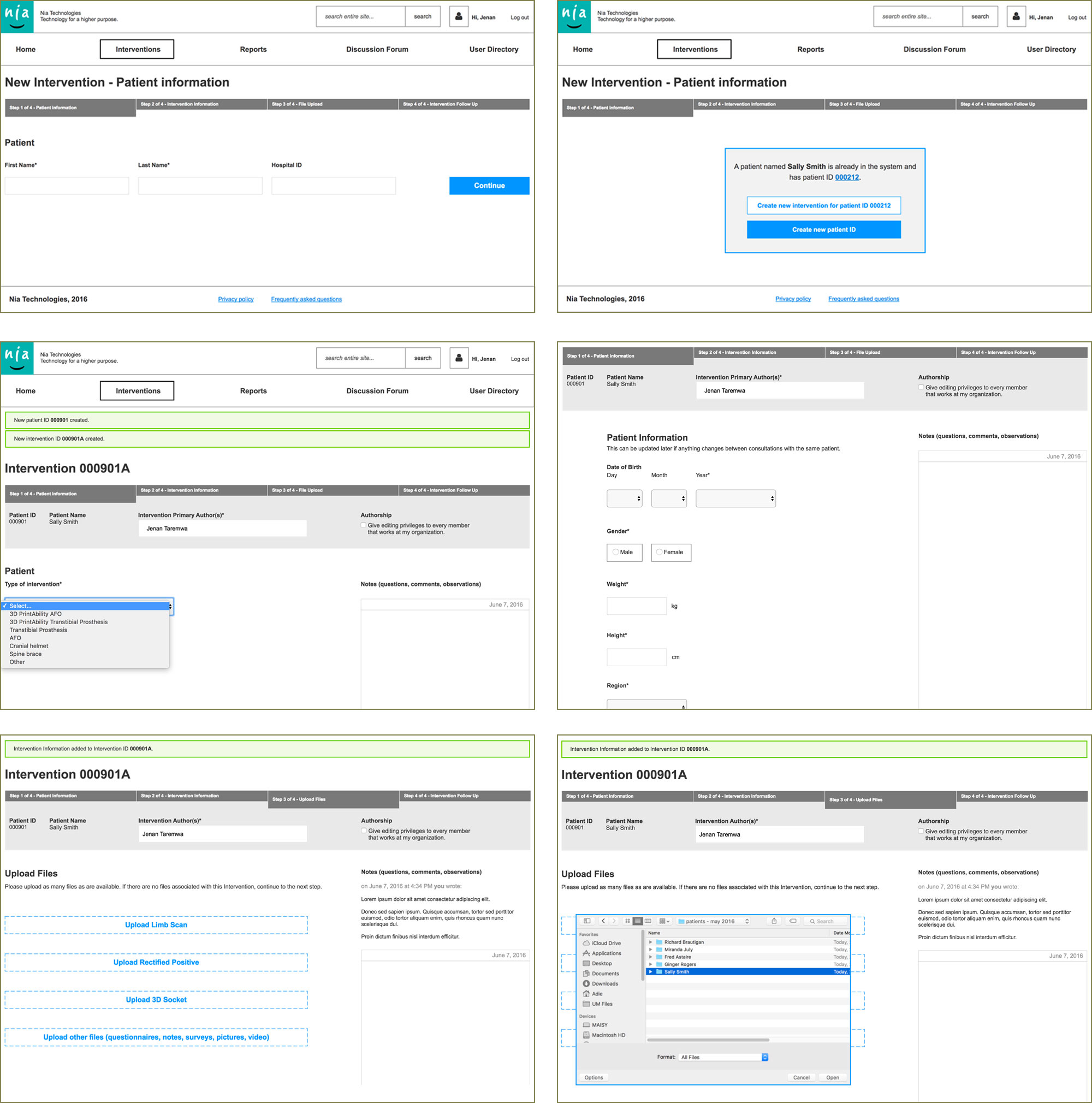
Figure 3.3
A sample of screens in the patient intervention data entry flow for the point of care practitioner.
Mandatory open form fields the user has to type into were kept to an absolute minimum.
The system would do the heavy lifting by asking for simple questions in drop downs (e.g. intervention type) then forking the upcoming questions based on the answers already provided. Progressive disclosure was consistently used to simplify data entry.
Dialogues providing the option to automatically batch data input or to consolidate multiple patient interventions would appear opportunely to save time and effort.
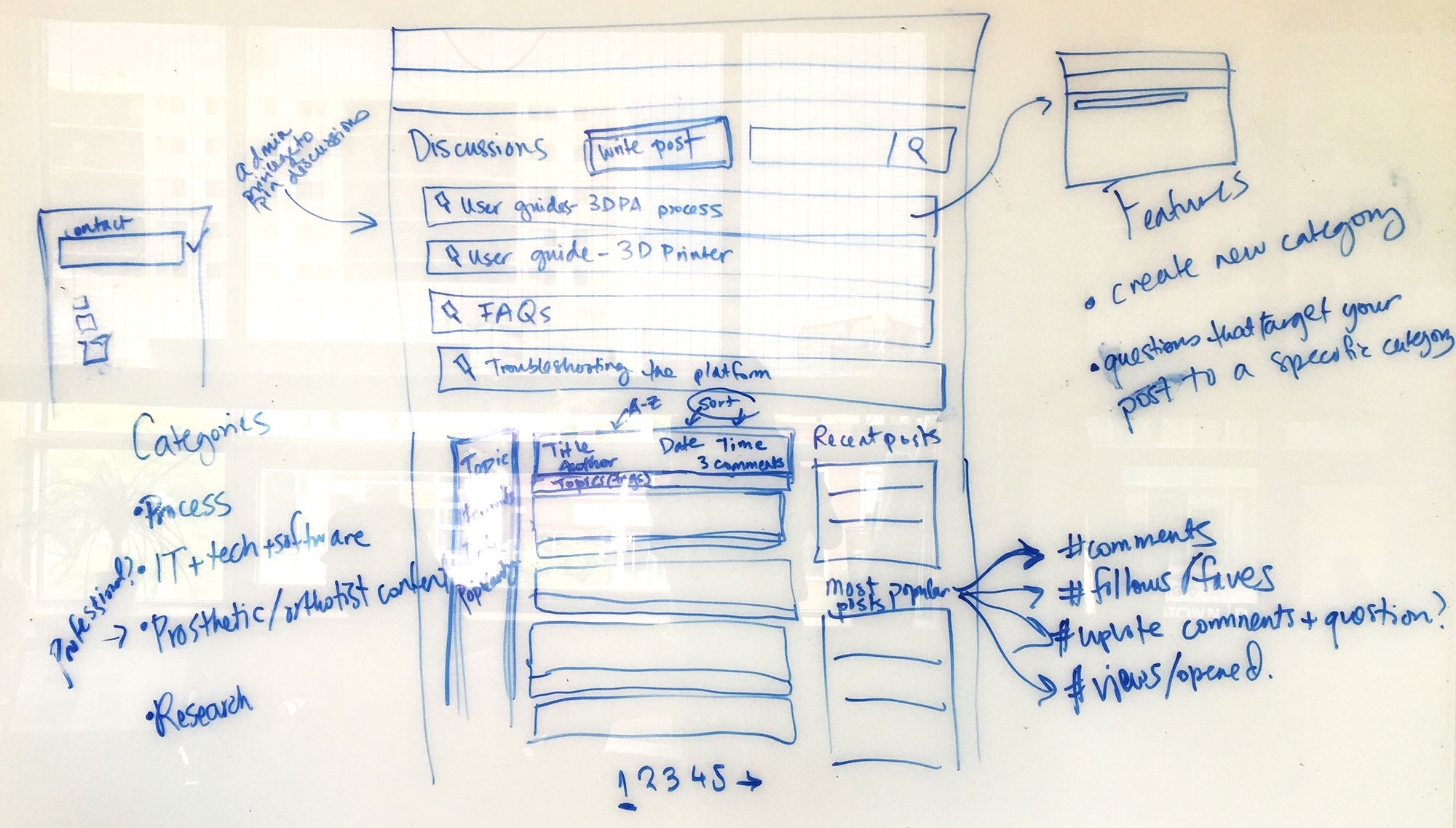
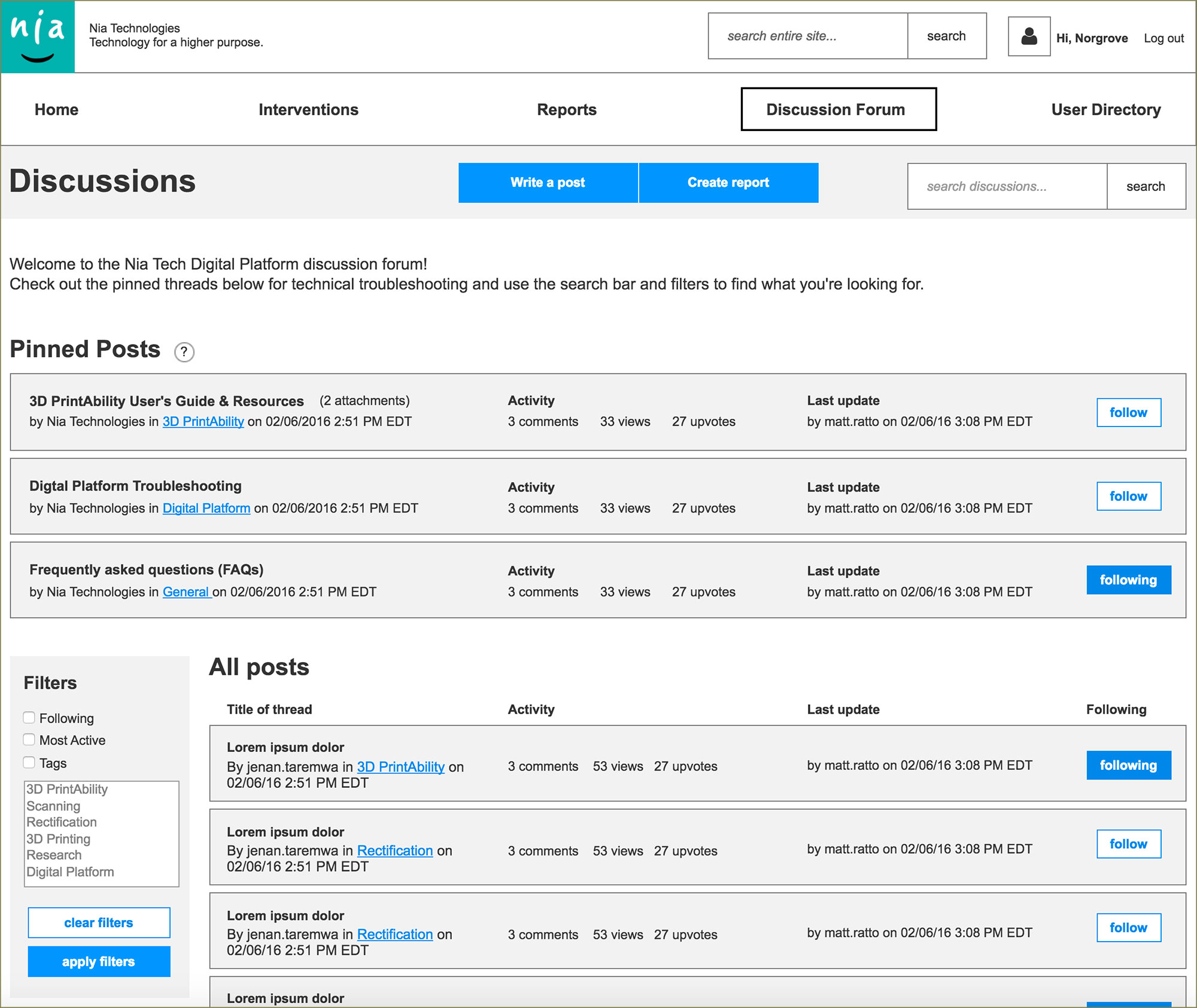
Figure 3.4
Sketch and Axure prototype page of the Discussion area of the platform.
Filtering and sorting posts by relevance, topic, and user’s own involvement were important features to consider and design for.
04
Evaluative Research and Design Iteration
We tested the Axure prototype with prosthetic technicians at Boundless Bracing and with Prosthetist/Orthotist clinicians and students at Sunnybrook Health Sciences Centre. Our overarching research objective was to ensure that our target users can successfully use the platform and can see value in it. We focussed on the researcher’s role of peer reviewing interventions and participating in forum discussions.

Figure 4.1
Evaluative usability testing at Boundless Bracing in Mississauga, Ontario. Our participants were Prosthetic/Orthotic clinicians, technologists and technicians.
Several participants expressed excitement at having a readily available online repository of peer support and documentation for innovative processes.
We also conducted usability testing training with the Nia team that would return to Uganda for a follow up 3D Printability study so that the technologists on-site could test the tool and give us additional insights on usability issues cross-culturally. These testing sessions focussed on data entry at the point of care.
Some of our findings led to improved affordance of buttons and CTAs in the tool, nomenclature changes in the navigation, and invalidated our assumption that people are used to scrolling in any web-based interface. In fact, when users differentiate a web-based tool from a website, they expect it to behave like any other off-line tool that has everything available in the viewport with minimal scrolling.
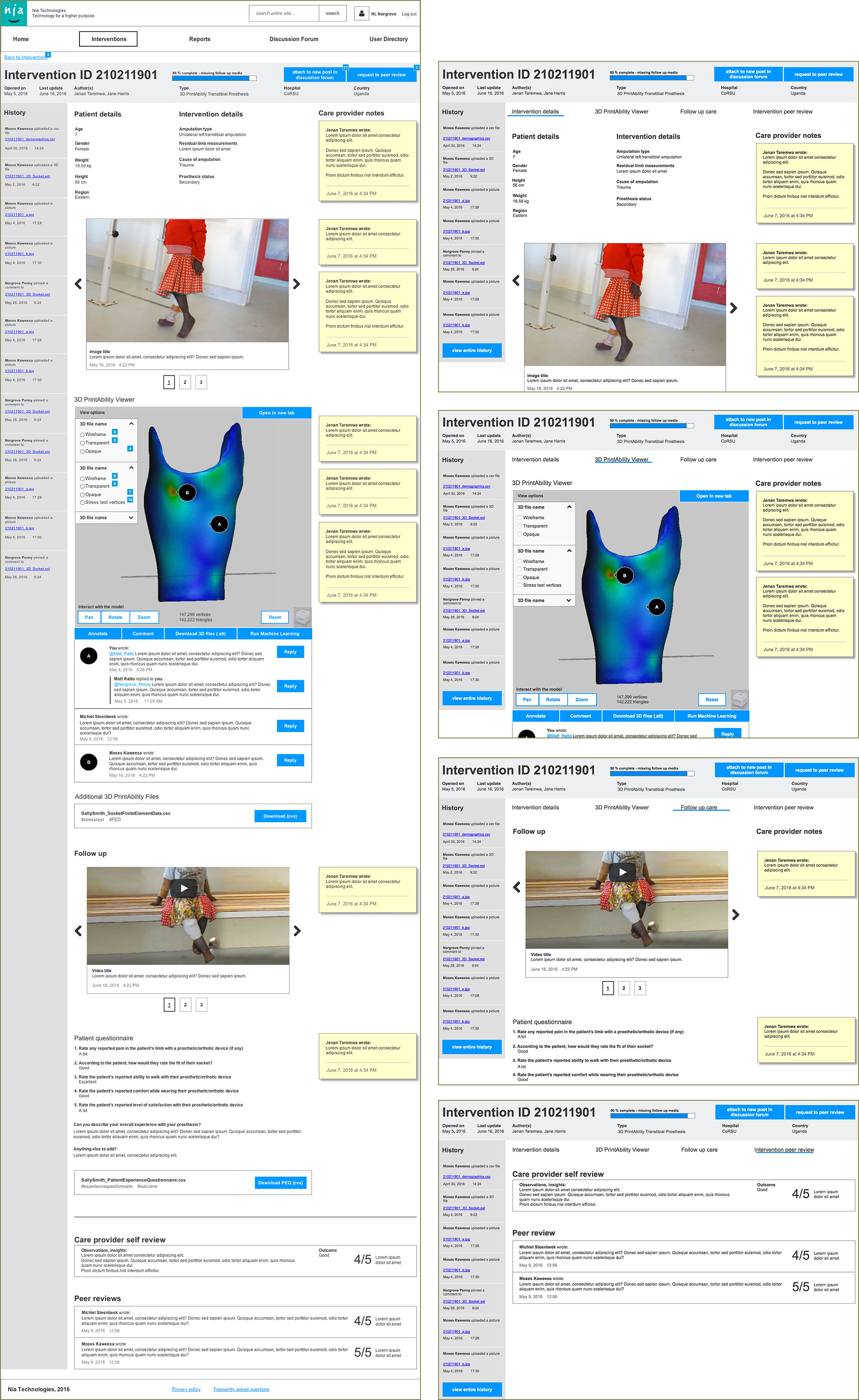
Figure 4.2
On the left: the design we tested with, a long scrolling page detailing all intervention information.
On the right: the iteration influenced by testing, where the different components of an intervention have been divided into four tabs that make all content available in the viewport with minimal scrolling.
05
Learnings
- ANever underestimate the importance of generative research in the planning stages for a new product.
What we heard from stakeholders, practitioners, and clinicians at the point of care was crucial in guiding our design decisions and providing a better solution for our client.
- BDelegating and project management is crucial when there are multiple locations, stakeholders, user groups, and diverging client/stakeholder priorities.
We could not have gotten insights from practitioners at the point of care in Uganda if we did not train members of the core client team to conduct user testing. We also could not have worked an aggressive timeline without delegating some of the UX design, local user testing and stakeholder interviews to members of the client team.
- CAccessible design is not just for people with disabilities - clinicians in dusty, very sunny prosthetics workshops needed to see the information on a screen.
With the aid of white backgrounds, high contrast elements, and large, readable fonts, we ensured they can perceive the information on the screen.
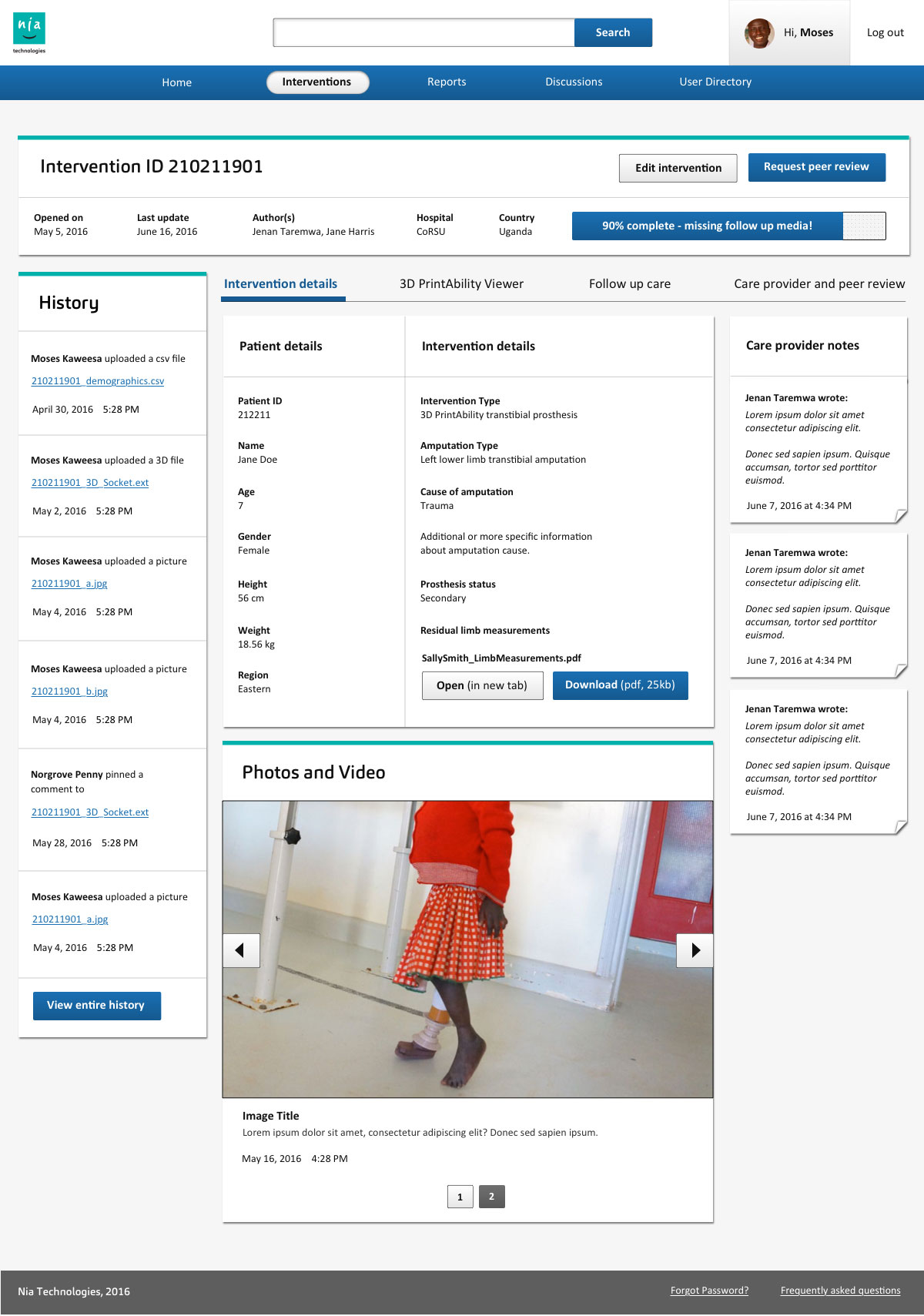
Figure 5.1
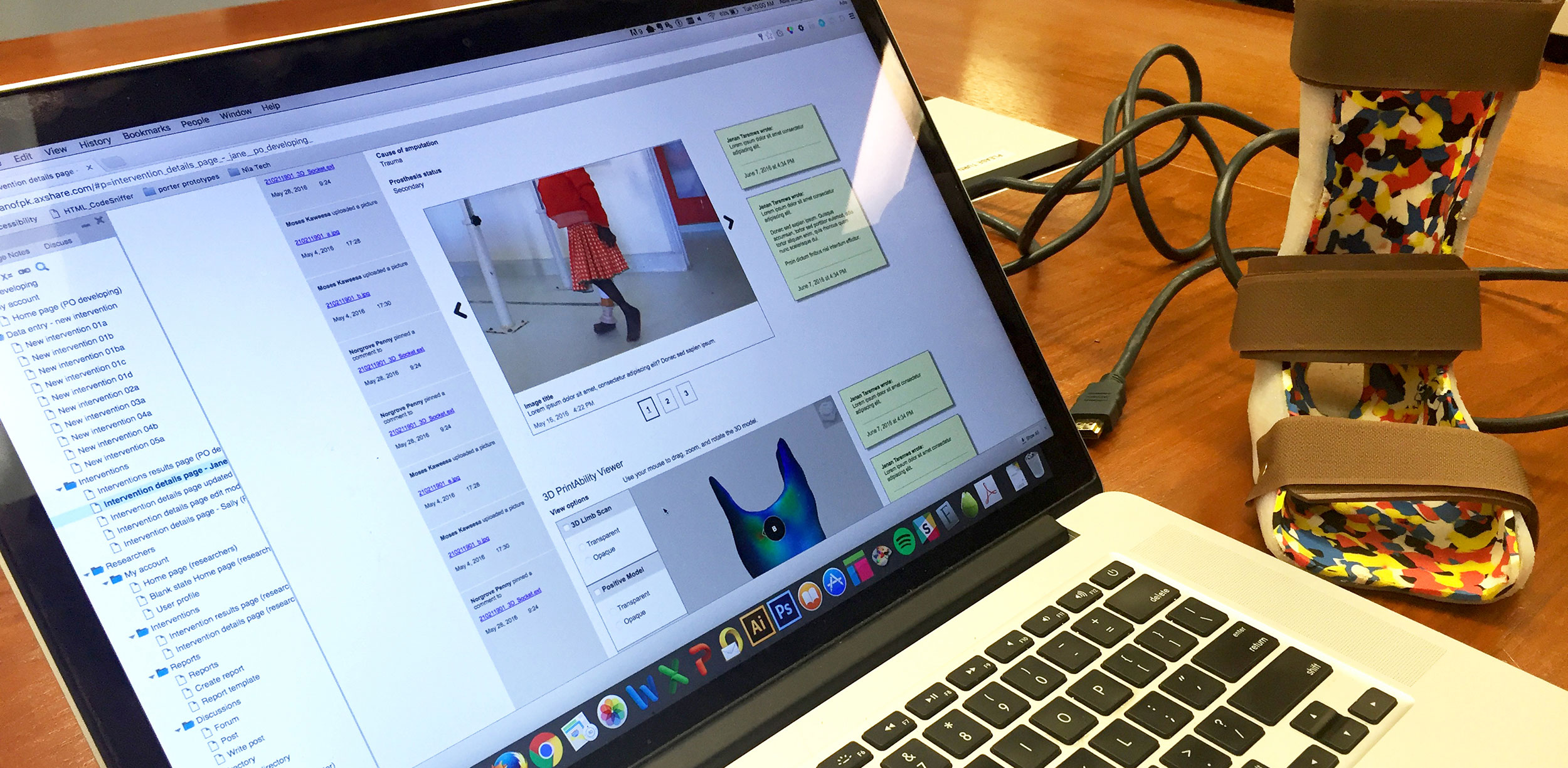
Visual design of an intervention page on the prosthetics data platform by Mel Banyard.
The visual design was influenced by usability testing and driven by accessibility to provide the best experience for users of different nationality, in different envirionmental contexts, with varying technological proficiency.
06
Impact
Client Testimonial
"Thanks to UM’s diligent planning, incisive questioning, and meticulous attention to detail, they helped us clarify what we were trying to achieve and what we needed in place to create a useful online tool. The UM team quickly developed an impressive understanding of P&O clinicians’ needs – with relevant knowledge of a sector that was new to them – and consistently delivered high-quality results. Ever professional, they were also fun to work with.
- Jerry Evans, President & CEO, Nia Technologies
The axure prototype was used as an alpha version of the product to secure continued funding from Google.
The prosthetics collaborative platform is currently being developed and Nia Technologies is accepting beta testers with prosthetic/orthotic domain expertise. To find out more, visit the Nia Technologies website.